
By Meredith Rief
For many, the United States represents a place of prosperity and opportunity. Globally, the United States ranks first in annual GDP, tops the list for the largest military, and ranks third in innovation. Despite boasting these advances over other nations, the United States often stumbles into last place when matched up against the healthcare systems of comparable developed countries.
In fact, when compared to ten other major developed nations, the US falls to the bottom of the list in almost every category including healthcare access, administrative efficiency, equity, and health outcomes for our population (Schneider et al., 2021). What’s the category that we rank first in? Health spending. While there are multifaceted reasons for the United State’s outlandish health spending, a core contributor is unrestricted prices on health commodities.
So why does a small vial of insulin cost nearly 100 dollars in the US while closer to 12 dollars in Canada, relatively? (Irving, 2021) The government in many other nations acts as a sole negotiator with large healthcare players to establish standard pricing for pharmaceutical drugs for a menu of healthcare procedures. In the United States, our system differs radically. Each individual insurance company acts as a small player negotiating with hospitals and the pharmaceutical industry to establish prices. With each insurance company having comparatively less leverage by representing a small proportion of consumers, prices are driven up.
As a result, in both dollar amount and proportion of GDP, the US consistently fits the bill for an astounding healthcare cost every year. In 2020, the United States spent a whopping 19% of its annual GDP on health consumption, with the next highest nation being the United Kingdom trailing behind at 13% of their annual GDP devoted to health spending (Wager et al., 20229.. See below how far of an outlier the US in comparison to our world’s counterparts when measuring health spending as a proportion of GDP.
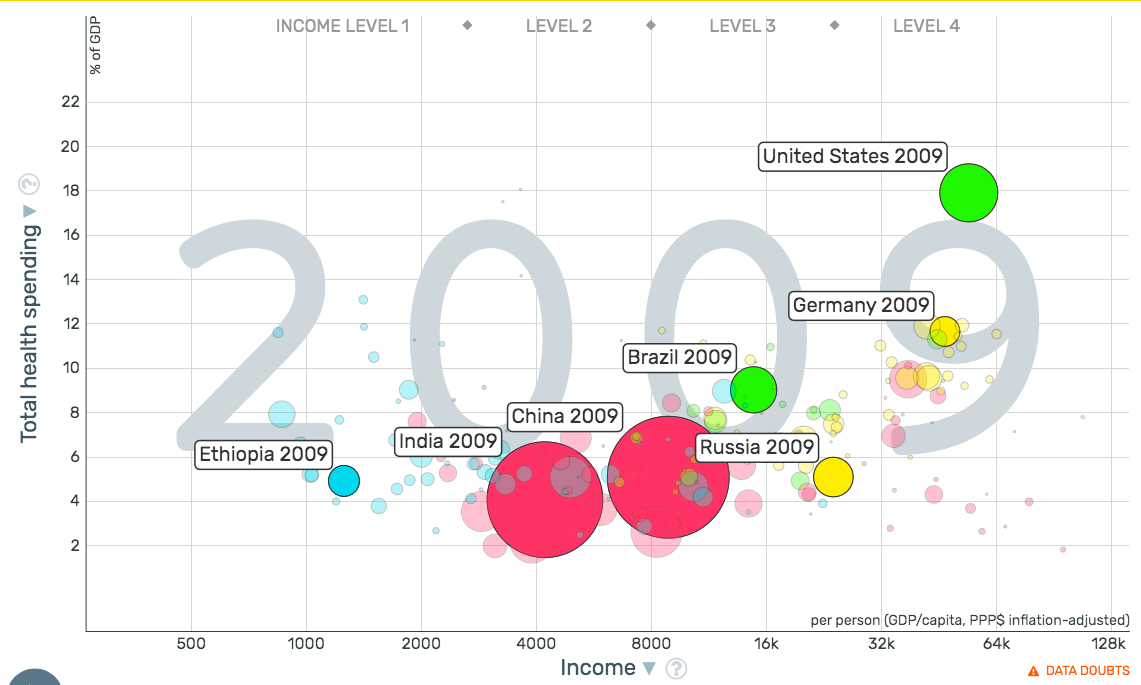
(Chart sourced from gapminder.org)
Despite our overblown budget for healthcare, the American people are sicker than ever compared to our developed nation’s counterparts. Nearly six in ten Americans have a chronic disease with four in ten having at least two (Center for Disease Control, 2022). Smoking, heart disease, obesity, and hypertension plague our country, with one in four deaths being attributable to heart disease. For many Americans, these health conditions compound throughout life resulting in both physical and financial distress in later adulthood.
Notably, the burden of both these health conditions and financial stress is not borne equally by our population. A growing body of literature focuses on the social determinants of health. This framework establishes that healthcare delivery is only one facet of our lives that contributes to making us more or less healthy. Other factors that contribute significantly to health are one’s environment, educational attainment, stable employment, access to nutritious food, as well as healthy social relationships.
One of the biggest predictors for lifelong health and life expectancy is economic well being, which is often associated with a host of other social factors that improve health throughout one’s life. The reasons for this relationship are complex and multifaceted, due to a combination of access to resources, lifestyle factors, and preventative care. Those with more financial resources typically rely on more nutritious food sources and living environments more conducive to healthy living. These disparities are reinforced by the structure of our healthcare system.
Since the 1940s, most Americans have relied predominantly on employer-based insurance to receive their healthcare. The implementation of this healthcare delivery system has provided numerous pros and cons. Providing insurance through the workplace allows for risk pooling which ultimately drives down the cost of insurance per individual. Typically, highly educated and high earning individuals are offered better insurance plans through their employer. Not only do these individuals have better health to begin with due to their socioeconomic status, these net benefits are reinforced with increased access to the best facets of our healthcare system. What is the net effect of these compounding factors? Health production is poured into many already healthy individuals where the marginal benefit to costly health interventions is fairly low. Those with adequate coverage receive regular checkups and preventative care which largely blocks the compounding of health conditions later in life.
In contrast, Americans with lower socioeconomic status not only need access to medical care the most, they are also the least likely to receive it adequately and consistently throughout their life. Unstable employment, less education, and lower paying jobs make the probability of receiving consistent and adequate care plummet. Much of our population would receive tremendous benefits of low-cost health interventions earlier in their lifespan. Simple checkups and preventative care can prevent health conditions from compounding later in life. Too often, diseases for low-income individuals are not addressed until they have compounded for decades and have become medical emergencies that are then addressed with costly interventions that may not even lead to significantly increased life expectancy.
The healthcare system in the United States is bleeding out both financially and in terms of efficiency. In the current privatized system, profit is maximized but our population’s health unfortunately is too often left out of this maximization equation. Frequently, those that need the least amount of care receive the most consistent access, while those that need the most care do not receive health interventions until much too late. This leaves the United States with a hefty bill, but inadequate health to show for our exorbitant spending.
References
“Chronic Disease Center (NCCDPHP).” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 21 Mar. 2022,
%20live,driver%20of%20health%20care%20costs.
“Health Equity Considerations and Racial and Ethnic Minority Groups.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html.
“How Does the U.S. Healthcare System Compare to Other Countries?” Peter G. Peterson Foundation,https://www.pgpf.org/blog/2020/07/how-does-the-us-healthcare-system-compare-to-other-countries.
Irving, Doug. “The Astronomical Price of Insulin Hurts American Families.” RAND Corporation, 6 Jan. 2021, https://www.rand.org/blog/rand-review/2021/01/the-astronomical-price-of-insulin-hurts-american-families.html.
Schneider, Eric C, et al. “Mirror, Mirror 2021: Reflecting Poorly.” Commonwealth Fund, 4 Aug. 2021, https://www.commonwealthfund.org/publications/fund-reports/2021/aug/mirror-mirror-2021
Wager, Emma, et al. “How Does Health Spending in the U.S. Compare to Other Countries?” Peterson-KFF Health System Tracker, 14 Feb. 2022, https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries-2/#:~:text=In%202020%2C%20the%20U.S.%20spent,from%2010%25%20in%202019).